 https://orcid.org/0000-0003-1327-3369
https://orcid.org/0000-0003-1327-3369
Introduction
Assessing health condition, level of hygiene and dietary habits is a fairly common practice in bioarchaeological studies (e.g., Ortner 2008; Yanko et al. 2021). This may allow researchers to draw conclusions about the lifestyle and socio-economic status of individuals or populations in certain historical periods. In this context, palaeopathological studies are interesting, because they show history of medical conditions and help us to better understand the aetiology of a disease. However, the diagnosis of pathology from bioarchaeological material is burdened with many limitations. This is because skeletal material is often destroyed and incomplete, knowledge about the life and health of a given individual/population is usually poor, and because many diseases have similar symptoms. As a result, it is rather difficult to recognise a specific disease, and thus indicating only potential causes of the destruction of bone material (Smith 2002; Ortner 2008). In this respect, case reports are informative by providing information regarding a presence of specific diseases in the past.
The aim of this study is to present the pathological lesions observed in a skeleton from Radom (Poland), dated to the 18th–19th century.
Materials and methods
The described skeleton comes from the Radom site, a medium-sized city located in central Poland, about 80 km from Warsaw (Fig. 1). The early medieval settlement complex in Radom consists of the ‘Piotrówka’ stronghold, the burial ground, and five open settlements. This complex was explored and partially examined in the second half of the 20th century by the Institute of the History of Material Culture of the Polish Academy of Sciences (now: Institute of Archaeology and Ethnology of the Polish Academy of Sciences) (Skubicha 2010). The results of these excavations have never been fully processed (Gąssowski 1951; Kierzkowska--Kalinowska 1970; 1979; Kurasiński and Skóra 2016; Baranowski et al. 2020).
Human remains were obtained during an excavation conducted in 2010–2013. The skeleton was found in the first urban municipal cemetery, which was founded at the stronghold in 1791. Due to the lack of space for new burials, the cemetery was closed and abandoned in 1811 (Zapłata 2011).

Fig. 1. The map of Poland with the location of Radom (black arrow)
The described human remains (No. 317/13) contained a fragment of splanchnocranium, with a fragment of right maxillary bone and the mandible. From the postcranial skeleton, the following parts were preserved: left and right forearms, both femurs, cervical and lumbar vertebrae and sacrum, both iliac and sciatic bones, and elements of ribs (Fig. 2).
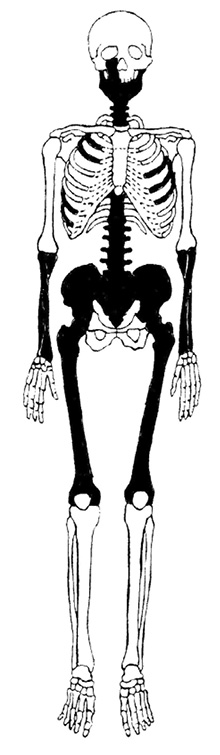
Fig. 2. Representation of the bones of individual No. 317/13 (present bones shown in grey)
The age-at-death of the individual was estimated on the basis of changes in the topography of the auricular surface (Buikstra and Ubelaker 1994; White and Folkens 2000). Moreover, it was possible to estimate the dental age-at-death using radiographic images of selected teeth (Drusini 2008). Age categories considered in the study were applied according to the following standards set by Buikstra and Ubelaker (1994): Young Adult (20–34 years), Middle Adult (35–49 years), and Old Adult (50+ years).
The referential sex of the individuals was estimated using the Phenice (1969) method. In addition, some mandibular features (expression of the mental eminence and gonion regions) were used in sex estimation (Buikstra and Ubelaker 1994; Konigsberg and Hens 1998; Walker 2008). Bone measurements were conducted according to the standards introduced by Buikstra and Ubelaker (1994), using a slide caliper and an anthropometric board.
Radiographical examinations were performed at the Forensic Medicine Department of the Medical University of Warsaw (Poland) using the Toshiba 16-slice computed tomography (CT) scanner and the X-ray Canon Radrex (Philips Medical System IEC 60601 X-ray, image – distance of 1 meter, in two perpendicular projections, 180-degree viewing angle used, horizontal frequency 47 kHz). The atypical juxtaposition of the femur with the hip joint on radiographs was used intentionally to better visualize the characteristic appearance of the femoral head with remodeling in necrotic lesions.
Results
The estimations of age-at-death and sex suggested that the individual being assessed was a male of about 35–38 years old.
Bone changes were observed in both femurs and both pelvic bones. The head of the femur is enlarged in a characteristic way (coxa magna); this deformation can be described as “mushroom-shaped”, with areas of smooth cortex, cavities, cystic residues. Subchondral cysts and porosity are present. Bony formations (osteophytes) on the femoral head margin are observed (Fig. 5–7).

Fig. 3. An anterior (photo above) and posterior view (phote below) of the femoral and coxa bones of individual No. 317/13 from Radom

Fig. 4. An anterior (left photo) and posterior view (right photo) of the femoral bones of individual No. 317/13 from Radom

Fig. 5. An anterior (left photo) and posterior view (right photo) of the proximal end of femoral bones of individual No. 317/13 from Radom. Photographs show a markedly flattened, “mushroom-shaped” femoral head, with areas of smooth cortex, cavities, cystic residues, porosity (white arrows), and osteophytes (black arrows)

Fig. 6. A posterior view of the proximals end of femoral bones of individual No. 317/13. Photographs show “mushroom-shaped” femoral heads, marginal osteophytes of femoral heads (black arrows)

Fig. 7. The deformities of femoral heads. Osteophytes (black arrows), the areas of smooth cortex, cavities, cystic residues, and porosities (areas in white circles) (No. 317/13)

Fig. 8. Femoral heads deformities; cavities, cystic residues, and porosities (No. 317/13). Left (left photo) and right (right photo) femoral bones; a porous surface is observed and the fovea capitis is disappeared (No. 317/13)
Both femoral heads are deformed, strongly flattened, and both are at a lower position than the greater trochanter (Fig. 3–6, 10). Length measurements of left femoral bone: measurement from the highest point of the greater trochanter to the lowest point of the medial condyle – 435 mm, measurement from the highest point of the femoral head to the lowest point of the medial condyle – 427 mm. The medial condyle damage made the adequate length measurements of the right femur was not possible. On both femoral heads the fovea capitis for the insertion of ligament teres were not observed (Fig. 7, 8). The neck of the femur is short and thick (upper-lower neck dimension: right bone – 35 mm, left bone – 40 mm; anterior-posterior neck dimension: right bone – 28 mm, left bone – 31 mm) (Fig. 3–6, 10). The femoral neck is almost nonexistent on the superior aspect (6 mm length on the left bone, 7 mm length on the right one) and greatly shortened inferiorly (18 mm length on the left bone, 17 mm length on the right one). Head center dislocated toward neck axis was not observed here. The rest of the bone (shaft and distal epiphysis) does not show any changes (Fig. 4).
The changes were also observed in both acetabularies of the hip joint. Right and left acetabulum is shallow, with marginal osteophytes and porosity on articular surfaces (Fig. 9). They also show subchondral bone remodelling (Fig. 10). Radiographic images show bilateral necrosis of the femoral head (Fig. 10). There is a significant sclerotization of the femoral head, with a discrete visible crescent sign.

Fig. 9. Left (left photo) and right (right photo) acetabulum with osteophytes (black arrows), cystic residues, and porosities (areas in white circles); the fovea capitis is disappeared (No. 317/13)

Fig. 10. Radiographs the femurs (proximal end) and pelvic bones with observable necrosis (white arrows) and osteophytes (black arrows) (No. 317/13)
Discussion and conclusions
The observed bilateral femoral head necrosis is idiopathic, and results from ischemic changes and bone remodelling. In patients, a symptom confirming the diagnosis of the vacuum phenomenon, caused by the release of nitrogen into the fissures in the head of the femur, which in turn accelerates the process of cyst formation in the area of the epiphyses. The macroscopic and radiological changes described match the symptoms associated with Legg-Calvé-Perthes disease (LCPD).
In the vast majority of reported cases, the disorder was found to be unilateral. For example, in less than 10% of cases, both hips are affected, and the joints are involved not simultaneously, but successively (Ortner and Putchar 1981; Leroux et al. 2018). In our case, necrotic changes are present in both femoral heads and both hips.
Generally, boys are affected about four times as often as girls. The condition is bilateral in between 10 and 20% of cases, although bilaterality is more frequently observed in girls (Guille et al. 1998; Pavone et al. 2019). This information is important for this case, as we are dealing with an adult male individual.
There is no consensus regarding the treatment of the disease, which is usually more focused on the prevention of femoral head collapse, progressive femoral head deformity and secondary degenerative arthritis, with restoring the range of motion and improving the functional recovery (Larson et al. 2012; Shah 2014).
Generally, the paleopathological evidence of LCPD are scarce. The disease has been previously described in: Peru (Ortner and Putchar 1981; Ortner 2003), Majorca (Marques and Cunha 2001), Serbia (Đurić et al. 2004), Czech Republic (Smrcka et al. 2009), Portugal (Ferreira et al. 2013), Argentina (Ponce and Novellino 2014), Egypt (Fritsch et al. 2015), China (Berger et al. 2017) and Spain (Manzon et al. 2017). Our study provides the first case of LCPD described in bioarchaeological materials from Poland.
A possible example of LCPD was diagnosed in the right femur of an adult female, which came from a miscellaneous group of femora accessioned as NMNH 265331 from the Valley of Chicama in Peru (National Museum of Natural History, Washington, D.C). The pathological changes observed on the femoral head were as follows: an obliterated depression for the ligamentum teres, a large circumscribed porous lesion covering more than half of the joint surface of the femoral head, bony overgrowth at the margins of the joint surface (a mushroom-like appearance), a depressed groove at the boundary with normal bone, a reduction in the mediolateral diameter of the head, bony outgrowths on the superior portion of the neck (Ortner and Putchar 1981; Ortner 2003). The pathological changes observed in the skeleton from Poland seem to be similar to the skeletal changes obtained from NMNH 265331 from Peru.
LCPD was found by Đurić et al. (2004) in a 30–40-year-old male skeleton from the medieval church of St. Ilija in the village of Ba, near Valjevo in western Serbia. In spite of some doubts, authors claimed that characteristics such as enlarged, malformed femoral head, thickening and shortening of the femoral neck, cyst-like destruction in the subarticular part of femoral head, irregular femoral head and acetabular surfaces, acetabular flattening, osteophyte formation on the upper margin of acetabulum suggest Perthes disease as the most likely diagnosis in this case
Smrcka et al. (2009), discussing the differential diagnosis of LCPD versus unilateral and bilateral osteochondroses of the femoral head in archaeological material and clinical situations, described two cases of archaeological LCPD from the Czech Republic. The first was a skeleton of a man older than 50 years, with the left hip affected (Langobard cemetery at Lužice in Moravia, dated to the late 5th century or early 6th century). The second case consists of a skeleton of an adult man from an archaeological investigation in Brandýsek (Bohemia; the 9th–10th century AD). Although authors emphasized that they were unable to exclude other causes of unilateral and/or bilateral osteochondrosis of femoral heads, they suggested these cases reflect Legg-Calvé-Perthes disease according to the criteria provided by Ortner and Putchar (1980). In both examined skeletal cases the following features were observed: mushroom shape of the femoral head, marginal osteophytes of the femoral head and acetabulum, greater trochanter evidently at a higher position than the center of the head, shallow, steep acetabulum, short and thick femoral neck. There was no substantial dislocation of the center of the femoral head from the axis of femoral neck, which also confirms that the authors were dealing with Perthes’ disease in the examined case. The head of the right femur was not preserved; therefore, it was not possible to determine whether it is unilateral or bilateral disorder (Smrcka et al. 2009). The pathological changes observed in the male skeleton from Radom are similar to those reported by Smrcka et al. (2004), which further supports our supposition that the male from Radom suffered from the LCPD disease.
LCPD symptoms were also diagnosed and described on the right femur and right hip bone in an adult male (50–60 years old, individual number 12) from Duratón Visigith necropolis in Segovia (Spain) (Herrerín and Garralda 2010). The skeletal characteristics, such as the length of the femoral neck, the radiologically observable trabecular disposition, the flattened and deformed, mushroom-shaped femoral head, and the absence of fovea capitis are described by authors as LCPD symptoms. In addition, the observed changes were supplemented to the attachment sites development on the whole skeleton to describe the individual’s mobility. Authors considered the obtained results, such as little muscular developmen on right femur, pronounced bilateral asymmetry observed in this individual’s tibiae, strong and deep marks of muscular attachments on the right humerus could indicate a frequent use of the right arm during movement, may suggest the LCPD disorder. Our case reports similar skeletal lesions to those described by Herrerín, Garralda (2010) which suggests the same disorder. In contrast to the Spain sample, however, in male skeleton from Radom muscle attachment sites are not strongly developed and do no differ between left and right bones. Nevertheless, this is not surprising given that in our sample both skeletal sides are affected, muscles are developed, or movement is limited symmetrically.
Lesions observed by Ferreira et al. (2013) in the right femur of an individual (no. 2) from the 15th–17th century cemetery in the Valle da Gafaria (Lagos, Portugal) are also compatible with the LCPD disorder. Initially, the authors diagnosed the observed symptoms as either LCPD or slipped femoral capital but ultimately classified them as Perthes’ disease. Slipped femoral capital epiphysis is a condition characterized by an inferior-posterior displacement of the femoral capital epiphysis, fusing with the neck in that position. The Legg-Calvé-Perthes disease do not exhibit such symptoms (Ferreira et al. 2013). The skeletal features observed in our sample are similar to the bone changes seen in an individual from Portugal (Ferreira et al. 2013) which further supports our diagnosis. The lack of inferior-posterior displacement of the femoral capital epiphysis in the Radom sample may also suggest the LCPD condition.
The observed in the Radom skeleton bony lesions, diagnosed as Legg-Calvé-Perthes disease symptoms, are similar to those observed in an individual from the Necropolis of Santa Maria, Sintra (Portugal), dated to the 14th–17th centuries (Wasterlain and Umbelino 2014). In this study, authors reported various macroscopic and radiological aspects as the most probable diagnosis of Legg-Calvé-Perthes disease in one of examined individual.
LCPD symptoms were also diagnosed by Ponce and Novellino (2014) in the well-preserved juvenile skeleton (individual (C 12), aged 14–16 at the time of death) from Argentina (late 16th to 17th century). Slipped capital femoral epiphysis and developmental dysplasia of the hip were excluded as potential causes of the skeletal condition, and the combined radiological, macroscopic, and osteometric examinations indicated that LCPD was the most likely diagnosis. “Mushroom-shaped”, deformed femoral head, its lower position according to the greater trochanter, the absence of the fovea capitis, short and wide femoral neck, wider, flattered, and irregular acetabulum these are the traits which authors to diagnose them as Perthes’ disease. The above characteristics were also observed in the skeleton from Radom.
Similar to our sample pathologies has also been identified in ancient Egyptian mummies from the Museum of Antiquities in Cairo by Fritsch et al. (2015), who examined orthopaedic diseases in Ancient Egypt, and by Manzon et al. (2017) who reported on morphometric and radiological analyses of a skeleton from the Etruscan necropolis of Spina (Ferrara, Italy, 6th–3rd century BCE). Similarly, Berger et al. (2017) examined skeletal remains of an individual from the Warring States period in Shaanxi Province (China), and observed a “mushroom head” deformity of the proximal right femur, an enlarged acetabulum, along with a contralateral tibia, talus as well as enlarged navicular with periosteal new bone formation. These conditions were also connected with LCPD.
As highlighted above, LCPD has been rarely reported in ancient populations, and its differentiation from other pathological changes in dry bones (aseptic necrosis in Gaucher’s disease, slipped femoral epiphysis) may be difficult (Wasterlain and Umbelino 2014) as all these conditions can produce similar lesions on the femoral head, making diagnosis difficult. Waldron (2009) suggested that the morphological changes associated with LCPD in human skeletal remains can include: a flattened mushroom-shaped femoral head with overhanging margins, thickening and shortening of the femoral neck along with a wide and shallow acetabulum, a normal position of the femoral head in relation to the axis. These femoral changes can be considered distinctive features of LCPD in palaeopathology.
As Waldron (2009) described, the LCPD condition passes through four stages: i/ the onset of avascular necrosis; ii/ femoral head fragmentation; iii/ revascularisation and regeneration; and iv/ healing. Late changes occurred in LCPD include: a shallow acetabulum and a smooth flattening of the femoral head, enlargement of the femoral neck and head, widening and shortening of the femoral neck with a varus deformity, mushroom deformity of the femoral head, shortening of the limb on the affected side, secondary osteoarthritis (Waldron 2009). We also observed such advanced changes in the examined individual from Radom.
LCPD is a complex disease affecting the epiphysis of the femoral head in the paediatric population. The disease occurs as avascular necrosis of the proximal femoral head that is a result of the tenuous blood supply to this area. The disorder is usually observed in boys at the age from 4 to 10 years (Loder and Skopelja 2011; Perry and Hall 2011; Pavone et al. 2019). Despite the aetiology of the disease having been widely discussed, it is still not fully understood (Hosalkar and Mulpuri 2012; Berger et al. 2017). The best supported theory involves an influence of repetitive mechanical stress on blood supply to the epiphysis (Guerado and Caso 2016; Leo et al. 2018).
At this stage of the analysis, it is not possible to determine the cause of LCPD in the Radom sample. Firstly, despite the aetiology of the disease having been widely discussed, it is still not fully understood (Hosalkar and Mulpuri 2012). The major hypothesis relies on a multifactorial genesis, involving genetic, mechanical, traumatic, metabolic, nutritional, environmental, hormonal, and hematologic conditions (Thompson and Salter 1986). Secondly, the archaeological and historical data concerning the examined individual are poor. Therefore, it is not possible to form a hypothesis about the aetiology of the disease. Archaeological and historical data about Radom and its population are available (e.g., Bogucka and Samsonowicz 1986; Kusiński 1991; Kozak 1997; Piątkowski 2000), but they cannot be directly related to a single individual. Although the sample provides some information about the health and biological condition of skeleton No. 317/13, it does not provide any data about this person’s individual lifestyle, which limits the possibility of formulating any hypotheses.
In conclusion, all the macroscopic and radiological changes observed and described in the examined male skeleton (No. 317/13) from Radom match the symptoms associated with Legg-Calvé-Perthes disease.
Acknowledgements
This research was funded by the National Science Centre (Poland) from 2013–2017 (Grant No 2013/11/B/HS3/04117).
Conflict of interest
Authors do not have any conflict of interest.
Authors’ contributions
AM: carrying out skeletal analyses, preparation and description of the manuscript; HM-P: carrying out skeletal analyses, preparation and description of the manuscript; ER: carrying out skeletal analyses, preparation and description of the manuscript; AD: carrying out skeletal analyses, preparation and description of the manuscript; JT: planning and supervision of the research, setting a goal, substantive supervision.

